Dear Doctor,
I must start this letter by saying I am exceedingly grateful to have had the opportunity to be treated by you. I recognize that you have studied Meniere's disease ad nauseum, published hundreds of articles about it, and traveled the world to attend and present at conferences on the subject. When I read about the struggle other sufferers have just in getting a diagnosis, much less appropriate treatment, I feel a bit guilty to have had the sheer luck of living close enough to be cared for by someone as competent as you.
But, as the person living with the frustrations of this disease, I feel compelled to tell you that I wish there was one more thing you would have encouraged me to do a long time ago: get a hearing aid.
Shortly after getting my last gent injection, it became apparent that my hearing had reached a new low, to the point that I now fell into the "severe hearing loss" category in that ear. I don't fault the gent, it gave me my life back by stopping the relentless vertigo I was experiencing. My hearing stunk before the gent anyway. So, at my follow-up appointment with you, I asked if I qualified for a hearing aid. You winced. I think you felt badly about the possibility that the gent may have stolen a little more sound from my world. I appreciate your compassion. You stated that some of your patients found that hearing aids made them feel dizzy. Considering what I had just been through, Lord knows I didn't want to do anything to make me feel dizzy. You also went on to say that hearing aids don't always help people with Meniere's disease due to the fluctuating nature of our hearing loss. All that being said, you kindly referred me to the audiologist in your office anyway. I must have looked pretty pathetic.
I met with the audiologist. A stoic woman, very matter-of-fact, but pleasant enough. She confirmed that my hearing loss was significant and proceeded to discuss a couple of models of hearing aids that might benefit me. After asking some technical questions, I asked about cost. I already knew my health insurance did not cover the expense of these little devices. She took a deep breath and said, "$1800 to $2000 - for one." Fortunately, I only needed one, but at that point I abruptly said I needed to think about it and walked out of her office, disgusted.
Three stikes: potential for dizziness, questionable benefit, and cost. So I groped for sound for the next two years. I kept a stiff upper lip while experiencing exhaustion, brain fog, hyperacusis, and further progression of my hearing loss. Somehow I managed.
Then last summer I had a new job opportunity handed to me on a silver platter. It was all but my dream job, working for a well-respected company and putting my years of professional experience to good use for the common good. This meant a new office with new coworkers. My previous employer and colleagues had lived my Meniere's journey with me and had been very accomodating. Coincidentally, my desk had been positioned such that my hearing environment was almost ideal and although I still had some difficulty hearing, I got by well enough. I had made the decision not to tell my new employer about my diagnosis. My interviewer informed me of the company's stringent physical exam requirements and an off-handed comment was made about a candidate who was once turned down for employment due to a heart murmur. As my current employer was going through some major changes at the time, which put into question my long-term job security, I felt I needed to do everything I could to secure this new job, so I didn't mention my hearing loss.
Two months into my new position, I was struggling terribly. Not only was I frequently asking people to repeat themselves, but I couldn't ask for any accomodations for my condition. Eventually, I did lightheartedly mention to a few people that I had some trouble hearing out of my right ear and could they please get my attention before speaking to me, but they quickly forgot and continued to talk to me with their head turned away from me or from behind my back. When I worked in the clinic with patients or taught group classes, I couldn't understand what was being said. I couldn't ignore my hearing loss anymore.
I'll skip the details of being evaluated and shopping for my hearing aid, but I eventually took the $1800 plunge and here's what I learned after getting this little beauty that I wish someone had told me sooner:
1. Stimulating the brain with sound improves hyperacusis, the condition of being hypersensitive to sound. It was hard the first few weeks, but I was persistent. Rarely did I take the hearing aid out, despite sound grating on my nerves at first. Eventually, the sensation virtually disappeared. Only recently did I read that avoiding sound actually makes hyperacusis worse. The brain becomes super sensitive to noise when it is deprived of sound stimulation.
2. Correcting single-sided hearing loss makes the brain feel more balanced. This is hard to understand until you experience it. Basically, I was always favoring my good ear, tilting, twisting, and relying on it to understand what and where sounds were.
3. A hearing aid helps drown out some of the annoyance of incessant tinnitus.
4. The cost of a hearing aid takes into account the multiple appointments with the audiologist usually required for adjusting the hearing aid, not only in the beginning, but for the life of the device. I have probably used up half the cost of the HA already with visits for fine tuning, excessive feedback, and questions that have arisen with day to day use. Considering this and the huge improvement in my quality of life that I've experienced, it feels like a bargain.
5. Hearing aids can most certainly help at least some patients with Meniere's disease, such as yours truly. My hearing isn't perfect, nor is my hearing aid ideal in all environments, but I most definitely hear better than I used to. I can sense where a sound is coming from more so than before. I ask people to repeat themselves far less often than I used to (a real plus for my family!). I can understand conversations better, even in noisy environments.
6. I did not experience any increase in dizziness. In fact, I felt more balanced and much less fatigued at the end of the day.
So, in hindsight, Doctor, I wish you had encouraged me from the very beginning to get a hearing aid. It seems you might have read an article or two along the way about the effects of hearing loss on the brain, as well as on the quality of life of people who are living with it. I understand, though, that you are in the trenches of this disease in your own way. You have focused your career on treating the worst this condition has to offer: vertigo, balance disorder, and extreme physical discomfort. I don't really fault you. But I hope in the future when the next patient asks you about the pros and cons of getting a hearing aid, you might have a more balanced discussion with them about some very real benefits that can be achieved by wearing a hearing aid. Most major manufacturers of hearing aids have a 30- to 90-day return policy. So what does your patient have to lose? What do they have to gain?
Respectfully,
Someone who lives with Meniere's disease
Wednesday, March 20, 2013
Wednesday, February 20, 2013
The Science Behind Addictive Junk Food
This post is not directly related to Meniere's but I think everyone can agree that following a healthy diet can only be good for us. However, making the decision to eat better can be difficult without enough motivation to do so. Being healthy is certainly one motivation, but for many of us it can wax and wane. Another motivator is to consider where we spend our money. Would you rather support farmers and industries that produce foods that are good for us or an industry whose sole goal is profit at any expense? If you need that kind of motivation, this article may do it for you. I am not going to copy and paste the whole thing here since it is so long, but I encourage everyone to read and share it.
The Extraordinary Science of Addictive Junk Food
By MICHAEL MOSS
Published: February 20, 2013 94 Comments
On the evening of April 8, 1999, a long line of Town Cars and taxis pulled up to the Minneapolis headquarters of Pillsbury and discharged 11 men who controlled America’s largest food companies. Nestlé was in attendance, as were Kraft and Nabisco, General Mills and Procter & Gamble, Coca-Cola and Mars. Rivals any other day, the C.E.O.’s and company presidents had come together for a rare, private meeting. On the agenda was one item: the emerging obesity epidemic and how to deal with it. While the atmosphere was cordial, the men assembled were hardly friends. Their stature was defined by their skill in fighting one another for what they called “stomach share” — the amount of digestive space that any one company’s brand can grab from the competition.
James Behnke, a 55-year-old executive at Pillsbury, greeted the men as they arrived. He was anxious but also hopeful about the plan that he and a few other food-company executives had devised to engage the C.E.O.’s on America’s growing weight problem. “We were very concerned, and rightfully so, that obesity was becoming a major issue,” Behnke recalled. “People were starting to talk about sugar taxes, and there was a lot of pressure on food companies.” Getting the company chiefs in the same room to talk about anything, much less a sensitive issue like this, was a tricky business, so Behnke and his fellow organizers had scripted the meeting carefully, honing the message to its barest essentials. “C.E.O.’s in the food industry are typically not technical guys, and they’re uncomfortable going to meetings where technical people talk in technical terms about technical things,” Behnke said. “They don’t want to be embarrassed. They don’t want to make commitments. They want to maintain their aloofness and autonomy.”
A chemist by training with a doctoral degree in food science, Behnke became Pillsbury’s chief technical officer in 1979 and was instrumental in creating a long line of hit products, including microwaveable popcorn. He deeply admired Pillsbury but in recent years had grown troubled by pictures of obese children suffering from diabetes and the earliest signs of hypertension and heart disease. In the months leading up to the C.E.O. meeting, he was engaged in conversation with a group of food-science experts who were painting an increasingly grim picture of the public’s ability to cope with the industry’s formulations — from the body’s fragile controls on overeating to the hidden power of some processed foods to make people feel hungrier still. It was time, he and a handful of others felt, to warn the C.E.O.’s that their companies may have gone too far in creating and marketing products that posed the greatest health concerns.
In This Article:
• ‘In This Field, I’m a Game Changer.’
• ‘Lunchtime Is All Yours’
• ‘It’s Called Vanishing Caloric Density.’
• ‘These People Need a Lot of Things, but They Don’t Need a Coke.’
The discussion took place in Pillsbury’s auditorium. The first speaker was a vice president of Kraft named Michael Mudd. “I very much appreciate this opportunity to talk to you about childhood obesity and the growing challenge it presents for us all,” Mudd began. “Let me say right at the start, this is not an easy subject. There are no easy answers — for what the public health community must do to bring this problem under control or for what the industry should do as others seek to hold it accountable for what has happened. But this much is clear: For those of us who’ve looked hard at this issue, whether they’re public health professionals or staff specialists in your own companies, we feel sure that the one thing we shouldn’t do is nothing.”
As he spoke, Mudd clicked through a deck of slides — 114 in all — projected on a large screen behind him. The figures were staggering. More than half of American adults were now considered overweight, with nearly one-quarter of the adult population — 40 million people — clinically defined as obese. Among children, the rates had more than doubled since 1980, and the number of kids considered obese had shot past 12 million. (This was still only 1999; the nation’s obesity rates would climb much higher.) Food manufacturers were now being blamed for the problem from all sides — academia, the Centers for Disease Control and Prevention, the American Heart Association and the American Cancer Society. The secretary of agriculture, over whom the industry had long held sway, had recently called obesity a “national epidemic.” Read more...
The Extraordinary Science of Addictive Junk Food
By MICHAEL MOSS
Published: February 20, 2013 94 Comments
On the evening of April 8, 1999, a long line of Town Cars and taxis pulled up to the Minneapolis headquarters of Pillsbury and discharged 11 men who controlled America’s largest food companies. Nestlé was in attendance, as were Kraft and Nabisco, General Mills and Procter & Gamble, Coca-Cola and Mars. Rivals any other day, the C.E.O.’s and company presidents had come together for a rare, private meeting. On the agenda was one item: the emerging obesity epidemic and how to deal with it. While the atmosphere was cordial, the men assembled were hardly friends. Their stature was defined by their skill in fighting one another for what they called “stomach share” — the amount of digestive space that any one company’s brand can grab from the competition.
James Behnke, a 55-year-old executive at Pillsbury, greeted the men as they arrived. He was anxious but also hopeful about the plan that he and a few other food-company executives had devised to engage the C.E.O.’s on America’s growing weight problem. “We were very concerned, and rightfully so, that obesity was becoming a major issue,” Behnke recalled. “People were starting to talk about sugar taxes, and there was a lot of pressure on food companies.” Getting the company chiefs in the same room to talk about anything, much less a sensitive issue like this, was a tricky business, so Behnke and his fellow organizers had scripted the meeting carefully, honing the message to its barest essentials. “C.E.O.’s in the food industry are typically not technical guys, and they’re uncomfortable going to meetings where technical people talk in technical terms about technical things,” Behnke said. “They don’t want to be embarrassed. They don’t want to make commitments. They want to maintain their aloofness and autonomy.”
A chemist by training with a doctoral degree in food science, Behnke became Pillsbury’s chief technical officer in 1979 and was instrumental in creating a long line of hit products, including microwaveable popcorn. He deeply admired Pillsbury but in recent years had grown troubled by pictures of obese children suffering from diabetes and the earliest signs of hypertension and heart disease. In the months leading up to the C.E.O. meeting, he was engaged in conversation with a group of food-science experts who were painting an increasingly grim picture of the public’s ability to cope with the industry’s formulations — from the body’s fragile controls on overeating to the hidden power of some processed foods to make people feel hungrier still. It was time, he and a handful of others felt, to warn the C.E.O.’s that their companies may have gone too far in creating and marketing products that posed the greatest health concerns.
In This Article:
• ‘In This Field, I’m a Game Changer.’
• ‘Lunchtime Is All Yours’
• ‘It’s Called Vanishing Caloric Density.’
• ‘These People Need a Lot of Things, but They Don’t Need a Coke.’
The discussion took place in Pillsbury’s auditorium. The first speaker was a vice president of Kraft named Michael Mudd. “I very much appreciate this opportunity to talk to you about childhood obesity and the growing challenge it presents for us all,” Mudd began. “Let me say right at the start, this is not an easy subject. There are no easy answers — for what the public health community must do to bring this problem under control or for what the industry should do as others seek to hold it accountable for what has happened. But this much is clear: For those of us who’ve looked hard at this issue, whether they’re public health professionals or staff specialists in your own companies, we feel sure that the one thing we shouldn’t do is nothing.”
As he spoke, Mudd clicked through a deck of slides — 114 in all — projected on a large screen behind him. The figures were staggering. More than half of American adults were now considered overweight, with nearly one-quarter of the adult population — 40 million people — clinically defined as obese. Among children, the rates had more than doubled since 1980, and the number of kids considered obese had shot past 12 million. (This was still only 1999; the nation’s obesity rates would climb much higher.) Food manufacturers were now being blamed for the problem from all sides — academia, the Centers for Disease Control and Prevention, the American Heart Association and the American Cancer Society. The secretary of agriculture, over whom the industry had long held sway, had recently called obesity a “national epidemic.” Read more...
Friday, February 15, 2013
More on Hearing Loss and Dementia
I posted recently about hearing loss and mental decline. Today I discovered author Katherine Bouton whose book, Shouting Won't Help, will be published on February 17th. While reading a little more about her, I came across the following article which goes a long way to validate what many of us with hearing loss, and Meniere's disease specifically, affectionately call brain fog. Though it is what I imagine dementia might feel like.
Could Hearing Loss and Dementia Be Connected?
Interview by PAM BELLUCK
Published: February 11, 2013
This interview has been edited and condensed for space.
PAM BELLUCK: I’m Pam Belluck, I’m a health and science writer for The New York Times. And this week, I am interviewing Katherine Bouton, who has been a long time editor for The New York Times and it now a contributing writer to our science section. And she has written a book called, “Shouting Won’t Help: Why I — and 50 Million Other Americans — Can’t Hear You.” And it’s a look into her own personal journey with hearing loss and a look into the research behind hearing loss. Katherine has written a piece that looks at a very interesting and surprising connection that some scientists have found between hearing loss and dementia. Katherine, first of all, welcome to the podcast, thank you for joining us.
KATHERINE BOUTON: Thank you very much.
MS. BELLUCK: And why don’t you tell us a little bit about what the scientists have found here.
MS. BOUTON: In studies over about the past…beginning in 2011 and continuing now—a new study was just published last month—is that there seems to be a strong association between hearing loss and both the earlier onset and more serious degree of dementia even with milder hearing loss, but especially with very severe hearing loss. For somebody like me who has a hearing aid and a cochlear implant but I still don’t hear very , this is alarming news.
MS. BELLUCK: All they have found at the moment is what’s called an association. So we don’t have any kind of causal connection—either that dementia either causing hearing loss or vice versa. But they do have three interesting theories about what could be happening. Could you lay those out for us?
MS. BOUTON: Okay, I should mention that the primary researcher on this is Frank Lin, who is at Hopkins and his database are two or three different long-term epidemiological studies. The first was based on the Baltimore Longitudinal Study of Aging. I went to see him after that first study was published and he had three things to offer.
The first made a lot of sense. It was that people with hearing loss tend to isolate themselves and isolation is a risk factor for dementia whether you’re hearing or hearing-impaired.
The second is something that he calls cognitive load — and which I call cognitive overload. What happens is that when you aren’t hearing very well, even with corrected hearing you’re trying so hard to hear the person that it makes it very hard to actually listen to what the person is saying. It’s very hard to absorb the information. When I did my interviews for this book – and I did a lot — I taped all of my interviews and I had someone else transcribe them because I couldn’t hear the tapes. I went and I got my transcriptions back I was constantly surprised by what I had asked, what I had heard, what they had answered. Every interview was like doing the whole thing fresh twice over.
The third possible explanation is the one that is most alarming and it’s the one that scientists like Dr. Lin and others are beginning to look at, and that’s that there’s an underlying pathological mechanism that has an influence on both hearing loss and dementia. It could be something environmental. It could be something genetic. They just don’t know.
These studies so far have relied on self-reported use of hearing aids. The next study that Dr. Lin is doing — he’s submitted a grant application now — is to specifically study how hearings aids are used, how often they are used, how carefully they were fitted, how much continual contact with the audiologist there is, whether the hearing-impaired person uses any assistive technology in addition to the hearing aids or the cochlear implant.
MS. BELLUCK: I’m interested in what you’re saying about corrected hearing. You are somebody wearing a hearing aid and a cochlear implant and according to the research that would not necessarily make a difference here. According to his research so far, people who are wearing hearing aids — it didn’t protect them from getting dementia. So does that tend to suggest some support for this idea that there being this underlying biological mechanism that might cause both?
MS. BOUTON: First they have to determine what the real relationship is between correcting hearing and the development of early or serious dementia. So far, the questions about the uses of hearing aids have been answered anecdotally by the participants in the study. What Frank Lin and his colleagues are going to do now is a serious prospective study about how people use their hearing aids, how often they use them, how well they were fitted, how often they go back and have them reprogrammed, where or not they use assistive devices like FM systems and looping, which in effect augment the use of hearing aids and implants — until they can really determine the role of hearing aids and the development of dementia the underlying causative factor remains a sort of outlying explanation.
MS. BELLUCK: An unanswered question. You open your piece with a kind of anecdote about your own sense of cognitive overload, as you call it.
MS. BOUTON: What happens is that you can’t really hear what the other person is saying and so you’re grasping for straws and basically trying to direct conversation in a way where you’ll be able to predict the answers.
I was at a party with my husband who is a literary editor and he was talking to a writer who I recognized and who I’ve met before, but who I figured didn’t remember me. And suddenly I found the two of us standing side by side. And this writer has had best-selling books and he’s very highly regarded and I have read his books and I wanted to talk to him about them. And I had a question about the second book — how it referred back to the first book.
And as I started the sentence I realized that I couldn’t remember the name of the second book and as I got half way through the sentence I realized I couldn’t remember the name of the first book either. So I stumbled through the sentence and said, ‘your first book, umm, umm, ummm…’ and he said — he gave me two choices. One of them I’d never heard of and of them was the book I was actually thinking of.
Last year, even, I would not have put myself in that situation. I would have just stayed home. I wouldn’t have gone to the party and that’s where isolation comes into this association with dementia as well because it’s very typical behavior just to say, this is too hard, it’s too embarrassing, I’d rather stay home and read a book.
MS. BELLUCK: Now, did you explain to him upfront that you have hearing loss and wouldn’t be able to hear him?
MS. BOUTON: I did, but I don’t have any visible signs of hearing loss and I tell people but I think they simply can’t comprehend what I’m saying. And this is one reason I wrote the book. It’s because I think people do not understand what so many people in the United States, and around the world for that matter, what their life is like on a daily basis. Serious hearing loss — it’s something you can’t just try it out for yourself. You can’t put earmuffs on and go outside and see what it’s like because it’s not just that you can’t hear, it’s that what you do hear is distorted. You hear every single thing that’s going on in the room, in addition to whatever you can grasp of the speaker’s voice. You hear some kinds of sounds louder than other sounds. In my case I mostly hear the things — like a glass being put down on the table is like an assault. So, going out is difficult.
Even now, I have a dog that I walk in the park a lot and somebody will say to me, ‘What’s your dog’s name?’ and I’ll say, ‘He’s three years old.’ [Laughter.] It’s windy in the park. It’s hard to hear when it’s windy because it makes noise on your hearing aid. But, I usually just guess what it is: ‘What’s your dog’s name?’ ‘How old is your dog?’ ‘What kind of dog is that?’ They all sound about the same to me. And I take a chance on getting it right — one out of three times.
MS. BELLUCK: Well, you’re doing a great job with this interview, which we are doing across a table probably separated by about four feet.
MS. BOUTON: Well, I’m looking directly at you. And being able to read lips and hear at the same time is the optimal way to hear. There’s a term for it, it’s called the McGurk-MacDonald effect. It means that you hear bi-modally, so that if you can hear, and see and even better, hear and see and read, as you would do in captions on a TV, your hearing is optimized.
MS. BELLUCK: So, just to circle back to the subject of this piece, which is dementia, I would imagine that that’s something of great concern to you, you’re 65 now. What are your thoughts about whether you have increased risk for yourself?
MS. BOUTON: Yes, I do worry about it. My mother, who has perfect hearing at 88, has very severe dementia. So I would worry about dementia anyway from a genetic perspective, but these studies have given me additional reason to worry about it.
MS. BELLUCK: Is there anything else you would like to add?
MS. BOUTON: First of all, the number of people with hearing loss in this country is astonishing. Approximately 48 million people in this country have hearing loss. Of these 48 million people in this country with hearing loss, from mild to profound, by far the majority have sensorineural hearing loss, which is the hair cells are damaged in your inner ear. And that causes eventual deafness. By far the majority of this kind of hearing loss can be avoided. It’s all noise-related hearing loss.
And one of the things I do in the book is talk about how noisy our society is. We have a real love affair with noise. If you’ve gone into any restaurant recently you’ll know how loud it is. If you were at the Super Bowl and you weren’t wearing earmuffs, you were probably deafened. Stadiums deliberately amp up the noise. Restaurants deliberately amp up the noise. It’s a very dangerous environment and unless we do something to control the amount of noise we’re exposed to on a daily basis, this rate of hearing loss is going to go on. And if these studies between hearing loss and dementia turn out to be accurate, as we get older that means a really considerable number of people having earlier and more serious dementia, which is — it’s bad for them, but it’s a huge cost factor in terms of public health.
MS. BELLUCK: Absolutely. Well, Katherine Bouton, thank you so much for joining us, for writing this article, which is fascinating and worrisome. Katherine Bouton is a former New York Times editor and currently a contributing writer to the science section. She’s author of the new book, “Shouting Won’t Help: Why I — and 50 Million Other Americans — Can’t Hear You.” Thanks so much.
MS. BOUTON: Thank you.
Could Hearing Loss and Dementia Be Connected?
Interview by PAM BELLUCK
Published: February 11, 2013
This interview has been edited and condensed for space.
PAM BELLUCK: I’m Pam Belluck, I’m a health and science writer for The New York Times. And this week, I am interviewing Katherine Bouton, who has been a long time editor for The New York Times and it now a contributing writer to our science section. And she has written a book called, “Shouting Won’t Help: Why I — and 50 Million Other Americans — Can’t Hear You.” And it’s a look into her own personal journey with hearing loss and a look into the research behind hearing loss. Katherine has written a piece that looks at a very interesting and surprising connection that some scientists have found between hearing loss and dementia. Katherine, first of all, welcome to the podcast, thank you for joining us.
KATHERINE BOUTON: Thank you very much.
MS. BELLUCK: And why don’t you tell us a little bit about what the scientists have found here.
MS. BOUTON: In studies over about the past…beginning in 2011 and continuing now—a new study was just published last month—is that there seems to be a strong association between hearing loss and both the earlier onset and more serious degree of dementia even with milder hearing loss, but especially with very severe hearing loss. For somebody like me who has a hearing aid and a cochlear implant but I still don’t hear very , this is alarming news.
MS. BELLUCK: All they have found at the moment is what’s called an association. So we don’t have any kind of causal connection—either that dementia either causing hearing loss or vice versa. But they do have three interesting theories about what could be happening. Could you lay those out for us?
MS. BOUTON: Okay, I should mention that the primary researcher on this is Frank Lin, who is at Hopkins and his database are two or three different long-term epidemiological studies. The first was based on the Baltimore Longitudinal Study of Aging. I went to see him after that first study was published and he had three things to offer.
The first made a lot of sense. It was that people with hearing loss tend to isolate themselves and isolation is a risk factor for dementia whether you’re hearing or hearing-impaired.
The second is something that he calls cognitive load — and which I call cognitive overload. What happens is that when you aren’t hearing very well, even with corrected hearing you’re trying so hard to hear the person that it makes it very hard to actually listen to what the person is saying. It’s very hard to absorb the information. When I did my interviews for this book – and I did a lot — I taped all of my interviews and I had someone else transcribe them because I couldn’t hear the tapes. I went and I got my transcriptions back I was constantly surprised by what I had asked, what I had heard, what they had answered. Every interview was like doing the whole thing fresh twice over.
The third possible explanation is the one that is most alarming and it’s the one that scientists like Dr. Lin and others are beginning to look at, and that’s that there’s an underlying pathological mechanism that has an influence on both hearing loss and dementia. It could be something environmental. It could be something genetic. They just don’t know.
These studies so far have relied on self-reported use of hearing aids. The next study that Dr. Lin is doing — he’s submitted a grant application now — is to specifically study how hearings aids are used, how often they are used, how carefully they were fitted, how much continual contact with the audiologist there is, whether the hearing-impaired person uses any assistive technology in addition to the hearing aids or the cochlear implant.
MS. BELLUCK: I’m interested in what you’re saying about corrected hearing. You are somebody wearing a hearing aid and a cochlear implant and according to the research that would not necessarily make a difference here. According to his research so far, people who are wearing hearing aids — it didn’t protect them from getting dementia. So does that tend to suggest some support for this idea that there being this underlying biological mechanism that might cause both?
MS. BOUTON: First they have to determine what the real relationship is between correcting hearing and the development of early or serious dementia. So far, the questions about the uses of hearing aids have been answered anecdotally by the participants in the study. What Frank Lin and his colleagues are going to do now is a serious prospective study about how people use their hearing aids, how often they use them, how well they were fitted, how often they go back and have them reprogrammed, where or not they use assistive devices like FM systems and looping, which in effect augment the use of hearing aids and implants — until they can really determine the role of hearing aids and the development of dementia the underlying causative factor remains a sort of outlying explanation.
MS. BELLUCK: An unanswered question. You open your piece with a kind of anecdote about your own sense of cognitive overload, as you call it.
MS. BOUTON: What happens is that you can’t really hear what the other person is saying and so you’re grasping for straws and basically trying to direct conversation in a way where you’ll be able to predict the answers.
I was at a party with my husband who is a literary editor and he was talking to a writer who I recognized and who I’ve met before, but who I figured didn’t remember me. And suddenly I found the two of us standing side by side. And this writer has had best-selling books and he’s very highly regarded and I have read his books and I wanted to talk to him about them. And I had a question about the second book — how it referred back to the first book.
And as I started the sentence I realized that I couldn’t remember the name of the second book and as I got half way through the sentence I realized I couldn’t remember the name of the first book either. So I stumbled through the sentence and said, ‘your first book, umm, umm, ummm…’ and he said — he gave me two choices. One of them I’d never heard of and of them was the book I was actually thinking of.
Last year, even, I would not have put myself in that situation. I would have just stayed home. I wouldn’t have gone to the party and that’s where isolation comes into this association with dementia as well because it’s very typical behavior just to say, this is too hard, it’s too embarrassing, I’d rather stay home and read a book.
MS. BELLUCK: Now, did you explain to him upfront that you have hearing loss and wouldn’t be able to hear him?
MS. BOUTON: I did, but I don’t have any visible signs of hearing loss and I tell people but I think they simply can’t comprehend what I’m saying. And this is one reason I wrote the book. It’s because I think people do not understand what so many people in the United States, and around the world for that matter, what their life is like on a daily basis. Serious hearing loss — it’s something you can’t just try it out for yourself. You can’t put earmuffs on and go outside and see what it’s like because it’s not just that you can’t hear, it’s that what you do hear is distorted. You hear every single thing that’s going on in the room, in addition to whatever you can grasp of the speaker’s voice. You hear some kinds of sounds louder than other sounds. In my case I mostly hear the things — like a glass being put down on the table is like an assault. So, going out is difficult.
Even now, I have a dog that I walk in the park a lot and somebody will say to me, ‘What’s your dog’s name?’ and I’ll say, ‘He’s three years old.’ [Laughter.] It’s windy in the park. It’s hard to hear when it’s windy because it makes noise on your hearing aid. But, I usually just guess what it is: ‘What’s your dog’s name?’ ‘How old is your dog?’ ‘What kind of dog is that?’ They all sound about the same to me. And I take a chance on getting it right — one out of three times.
MS. BELLUCK: Well, you’re doing a great job with this interview, which we are doing across a table probably separated by about four feet.
MS. BOUTON: Well, I’m looking directly at you. And being able to read lips and hear at the same time is the optimal way to hear. There’s a term for it, it’s called the McGurk-MacDonald effect. It means that you hear bi-modally, so that if you can hear, and see and even better, hear and see and read, as you would do in captions on a TV, your hearing is optimized.
MS. BELLUCK: So, just to circle back to the subject of this piece, which is dementia, I would imagine that that’s something of great concern to you, you’re 65 now. What are your thoughts about whether you have increased risk for yourself?
MS. BOUTON: Yes, I do worry about it. My mother, who has perfect hearing at 88, has very severe dementia. So I would worry about dementia anyway from a genetic perspective, but these studies have given me additional reason to worry about it.
MS. BELLUCK: Is there anything else you would like to add?
MS. BOUTON: First of all, the number of people with hearing loss in this country is astonishing. Approximately 48 million people in this country have hearing loss. Of these 48 million people in this country with hearing loss, from mild to profound, by far the majority have sensorineural hearing loss, which is the hair cells are damaged in your inner ear. And that causes eventual deafness. By far the majority of this kind of hearing loss can be avoided. It’s all noise-related hearing loss.
And one of the things I do in the book is talk about how noisy our society is. We have a real love affair with noise. If you’ve gone into any restaurant recently you’ll know how loud it is. If you were at the Super Bowl and you weren’t wearing earmuffs, you were probably deafened. Stadiums deliberately amp up the noise. Restaurants deliberately amp up the noise. It’s a very dangerous environment and unless we do something to control the amount of noise we’re exposed to on a daily basis, this rate of hearing loss is going to go on. And if these studies between hearing loss and dementia turn out to be accurate, as we get older that means a really considerable number of people having earlier and more serious dementia, which is — it’s bad for them, but it’s a huge cost factor in terms of public health.
MS. BELLUCK: Absolutely. Well, Katherine Bouton, thank you so much for joining us, for writing this article, which is fascinating and worrisome. Katherine Bouton is a former New York Times editor and currently a contributing writer to the science section. She’s author of the new book, “Shouting Won’t Help: Why I — and 50 Million Other Americans — Can’t Hear You.” Thanks so much.
MS. BOUTON: Thank you.
Shouting Won't Help by Katherine Bouton
Here's a link to a new book coming out in 2 days called Shouting Won't Help, by Katherine Bouton. I just listened to this interview with her on NPR. Very fascinating, I can't wait to read the book.
Here is also a link and some excerpts to a NY Times article written by Bouton in August, 2012.
Excellent description of what those of us with hearing loss actually hear everywhere we go:
In a noisy environment like a restaurant, a person with normal hearing will still be able to hear his companion. But in that same environment, a hearing-impaired person will hear chairs scraping, dishes clanking, waiters shouting, all of it bouncing off the high ceilings, the bare walls, the chic metallic tables and chairs — an anxiety-provoking wall of noise. Worst of all is the restaurant’s background music, sometimes competing with a different sound track throbbing in the kitchen.
Earlier this week I had dinner with my husband and sister (both with normal hearing) and my daughter, son and niece, all 20-somethings, in a popular Brooklyn restaurant. It was my birthday and I had a great time, enjoying my family and the good food, but I didn’t hear one word said at the table.
Frustrating and exhausting...
Here is also a link and some excerpts to a NY Times article written by Bouton in August, 2012.
Excellent description of what those of us with hearing loss actually hear everywhere we go:
In a noisy environment like a restaurant, a person with normal hearing will still be able to hear his companion. But in that same environment, a hearing-impaired person will hear chairs scraping, dishes clanking, waiters shouting, all of it bouncing off the high ceilings, the bare walls, the chic metallic tables and chairs — an anxiety-provoking wall of noise. Worst of all is the restaurant’s background music, sometimes competing with a different sound track throbbing in the kitchen.
Earlier this week I had dinner with my husband and sister (both with normal hearing) and my daughter, son and niece, all 20-somethings, in a popular Brooklyn restaurant. It was my birthday and I had a great time, enjoying my family and the good food, but I didn’t hear one word said at the table.
Frustrating and exhausting...
Tuesday, February 12, 2013
Young Basketball Player with Meniere's Disease
Kaela Davis takes a temporary timeout
Feb 12, 2013 11:34 AM ET | By Walter Villa
Kaela Davis has always had the ability to score virtually any time she wanted on the basketball court.
But now is not that time.
Davis, a Georgia Tech recruit and the No. 2 prospect in the espnW HoopGurlz Top 100 for 2013, has left the Buford (Ga.) team for the rest of the season to get treated for Meniere's disease, an inner-ear disorder characterized by hearing loss and vertigo.
"Every day for a week I tried to convince my parents that I could make my doctors' appointments and still play basketball," Davis said.
She finally realized, however, that her condition is serious and must be addressed immediately. She has been dealing with Meniere's since she was 11 and has permanently lost about 90 percent of her hearing in her left ear. She hasn't played since a Buford loss Jan. 26.
"Now we're concerned about her other ear," said her father Antonio Davis, a former NBA All-Star. "This is something we've never discussed publicly before. We don't want pity for our daughter. But we felt it was something we had to address now because of the decision to pull her from the team."
“
One day when she has a family of her own, I want her to be able to hear her baby cry.
”
-- Kendra Davis
The 6-foot-2 Davis, who is expected to be named a McDonald's All-American later this week, plans to play in that game as well as at Georgia Tech next season. The two-time USA Basketball gold medalist was hoping to add a third state title to her résumé this year after winning one at Norcross (Ga.) as a freshman and then another at Buford as a sophomore.
Davis has been battling vertigo once or twice a year, although lately, symptoms of Meniere's have been occurring more frequently.
"It's like someone spins you around quite a few times -- how do you feel then?" she said. "Well, that's how I would feel for 24 hours [when the vertigo hits.]"
Her migraines also make her feel nauseous.
"When I get those headaches," Davis said, "every little movement hurts."
Davis admits she was emotional and "not very mature" when her parents told her she would have to give up a chance at a third state title.
"I understand her disappointment," said her mother, Kendra. "But one day when she has a family of her own, I want her to be able to hear her baby cry."
Now that she has had time to think about it, Davis is on board with her parents' wishes.
"It was a hard decision to make, but I have to worry about myself at some point," she said. "Let's take a step back, figure out what's going on and get a grip on it before it gets worse."
That's a very rational thought process, which is not surprising once you get to know her parents.
Antonio was a 6-9 forward for four NBA teams from 1993 to 2006, making the 2001 All-Star Game while with Toronto. He also served as the president of the NBA Players Association and currently works as an NBA studio analyst for ESPN.
Kendra is an interior designer and events planner who also is well versed in basketball, if only, she said, "by osmosis."
[+] Enlarge
USA Basketball
Kaela Davis has won two gold medals with USA Basketball and two state championships in high school.
The couple has two children, Kaela and her 6-8 twin brother A.J., who plays basketball for Buford and has signed with Tennessee.
The twins are best friends even though they are opposites.
"A.J. is way more outgoing and social," Antonio said. "Kaela is more quiet and introverted."
Davis had at one point committed to joining A.J. at Tennessee, the school she grew up rooting for because it's the alma mater of close family friend Candace Parker, who now stars for the WNBA's Los Angeles Sparks.
But after Tennessee's Pat Summitt announced she could no longer coach because of early onset dementia, Davis made another excruciatingly difficult decision by choosing to reopen her recruitment.
"It's the hardest and bravest thing I've seen her do," her mother said. "The new coaches at Tennessee are amazing and wonderful, but it's not quite the same thing [as Summitt]."
Davis had to restart her search from scratch.
As it happened, she wants to study engineering, and Georgia Tech, considered an excellent school in the field, is located within minutes of her Atlanta home.
Antonio said he is thrilled that -- unlike many NBA dads -- he has been around to see "tons" of his children's games. And when he sees Kaela, he comes away impressed.
"With her size and quickness and her basketball IQ, it allows her to do a lot of different things," he said. "I've seen her run the point, shoot 3-pointers and guard small forwards.
"She is very versatile, but I think she is most comfortable as a scorer, coming off screens and shooting the ball."
Davis, who is averaging 21 points per game, can score virtually any time she wants, her dad said, but just not right now.
"Her health is the most important thing," he said. "I don't want her to deal with this for the rest of her life. This is something we need to address now."
http://espn.go.com/espnw/hoopgurlz/8939194/georgia-tech-recruit-kaela-davis-sit-rest-senior-season-treat-meniere%20s-disease
Saturday, February 9, 2013
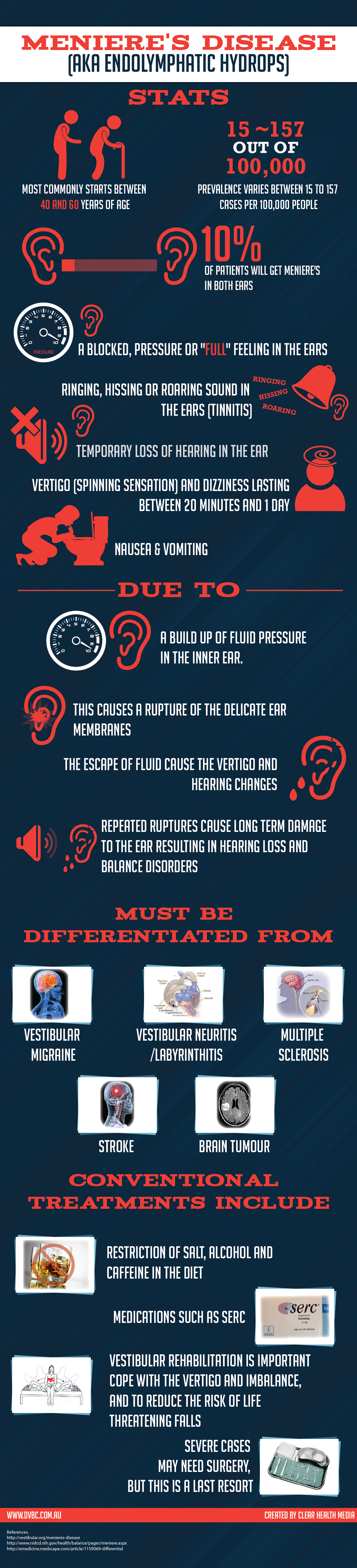
Great Meniere's Infographic
This can be found at:
http://dvbc.com.au/free-infographic-menieres-disease-aka-endolymphatic-hydrops
http://dvbc.com.au/free-infographic-menieres-disease-aka-endolymphatic-hydrops
Wednesday, February 6, 2013
Anxiety and Balance Disorders Could Be Linked
Thought-provoking studies. Go here for access to the links to the abstracts.
Balance and Anxiety
Posted on February 6, 2013 | Comments Off
Studies show that the body’s balance system is involved in anxiety disorders. Could treating vestibular problems lead to anxiety relief? That’s a subject that needs to be researched further.
References:
Autorotation test abnormalities of the horizontal and vertical vestibulo-ocular reflexes in panic disorder. (Link)
Panic disorder: the role of the balance system. (Link)
Relationship between balance system function and agoraphobic avoidance. (Link)
Serotonergic modulation of the balance system in panic disorder: an open study. (Link)
Space and motion discomfort and abnormal balance control in patients with anxiety disorders. (Link)
Visually induced postural sway in anxiety disorders. (Link)
Balance and Anxiety
Posted on February 6, 2013 | Comments Off
Studies show that the body’s balance system is involved in anxiety disorders. Could treating vestibular problems lead to anxiety relief? That’s a subject that needs to be researched further.
References:
Autorotation test abnormalities of the horizontal and vertical vestibulo-ocular reflexes in panic disorder. (Link)
Panic disorder: the role of the balance system. (Link)
Relationship between balance system function and agoraphobic avoidance. (Link)
Serotonergic modulation of the balance system in panic disorder: an open study. (Link)
Space and motion discomfort and abnormal balance control in patients with anxiety disorders. (Link)
Visually induced postural sway in anxiety disorders. (Link)
Monday, February 4, 2013
Meniere's Disease and Quality of Life Study
This study was published 13 years ago, coincidentally, by my local neurotologist, Jeffrey Harris. Next time you're wondering if having Meniere's disease is really as bad as it feels, you can turn to this small study for some validation. Fortunately, my own quality of life is pretty good right now but it hasn't always been this way and I expect someday it may take a nosedive again. On top of everything else, Meniere's is an unpredictable disease, sometimes misleading you to believe you might just have beaten it. I don't know whether this is a blessing or a curse. Anyway here's the study:
Released: 5/13/2000 12:00 AM EDT
Embargo expired: 5/12/2000 12:00 AM EDT
Source Newsroom: American Otological Society (AOS)
Release: May 12, 2000
Contact: Kenneth Satterfield, 407-238-4161 (as of 5/12/2000)
Meniere's Disease Leads to a Significant Decline in
Quality of Life for Patients with Disorder
A University of California-San Diego study highlights disease's impact on physical and mental health
Orlando, FL -- Meniere's disease is a chronic illness that often affects individuals in the prime of life. Many believe the disorder has a serious impact on the psychosocial status of individuals and their families. For the first time, a new study quantifies health-related quality of life status of patients with Meniere's disease who have failed conventional medical therapy and are candidates for further intervention and compares their status with other medical disorders described in a similar fashion.
Early studies suggested that there was a psychosomatic component in the etiology of this disorder. Now, it is generally accepted that the psychological aspects of the illness are in fact the consequence of the disease itself. A number of studies have shown Meniere's disease is associated with anxiety, depression and inability to concentrate.
The authors of the study, "Impact of Meniere's Disease on Quality of Life," are Jeffrey P. Harris, MD, PhD, from the Division of Otolaryngology-Head & Neck Surgery, and John P. Anderson, PhD, Department of Family and Preventive Medicine, at the University of California-San Diego. Their findings were presented before the American Otologic Society, meeting May 13-15, in Orlando, FL.
Methodology: Nineteen patients (12 female, seven male, age 32 to 83 yrs); all had been diagnosed with Meniere's disease that had been resistant to medical therapy; the baseline interviews on the subjects were performed by trained interviewers prior to any medical intervention.
Three instruments were used in the study:
Quality of Well-being Scale (QWB): A quantitative general health measure that allows for comparison of all diseases or conditions. It permits an analysis of programs, policies and treatments for the specified diseases and conditions, and allows calculation of Quality-Adjusted Life Years gained or lost by affected individuals. Patients are asked about their experience and dysfunction for each of the past six consecutive days. They are asked to define their symptom/problem complex - (headache, dizziness, ringing in ears), using criteria such as mobility scale-e.g. limitations in travel, physical activity scale-e.g. in bed, and social activity scale- e.g. working, housework.
Medical Outcomes Study SF-12: Widely employed general health status measure. This research tool rates physical and mental status by asking how often or how troublesome described situations are either during the past week or ongoing.
Center for Epidemiologic Studies-Depression Scale (CES-D): This is a widely used measure of psychological depression. Generally, 20 items rated on a scale of 0-3 over the past week: zero (best) to 60 (worst). Scores 16 or above indicate clinically significant depression).
Results: The study revealed the following:
-- QWB scores: Meniere's patients achieved a mean score of .505 on days of acute episodes and .620 on days without acute episodes. This compares with scores of normal adults (.810), very ill adults with life-threatening illness (cancer, AIDS (.616), non-institutionalized Alzheimer's patients (.506), and AIDS & cancer patients, six days before death (.427). This indicates that Meniere's patients lost 43.9% from optimum well-being or .439 quality adjusted life years lost for each year in their QWB state. This score reflects major impairment in mobility, physical activity, social activity and clear thought processes.
-- CES-D scores: Meniere's patients registered a mean CES-D score of 23 (significant depression 16 and above). This compares with trauma patients (CES-D 20), cochlear implant candidates (CES-D 15), patients with post-cochlear implantation (CES- D 12).
-- SF-12 scores: Meniere's patients recorded scores SF-12 physical- 38.9 (mean 50, + 10) and SF-12 mental- 44.2 ( mean 50, + 10). Meniere's disease patients are among the most severely impaired non-hospitalized patients studied thus far. These patients exhibit even more impairment on days with acute episodes. Patients describe impairment in travel, ambulation, work and other major social roles as well as trouble learning, remembering and thinking clearly. They are clinically depressed as a group.
Conclusions: The degree of impairment and depression which stems from this condition becomes the responsibility of treating physicians to develop and offer treatment options to their Meniere's patients. The authors call on the medical community and fellow specialists to not condone a nihilistic approach to treatment, stress to primary care colleagues that this condition requires treatment, and seek out effective treatment strategies for this debilitating illness.
Released: 5/13/2000 12:00 AM EDT
Embargo expired: 5/12/2000 12:00 AM EDT
Source Newsroom: American Otological Society (AOS)
Release: May 12, 2000
Contact: Kenneth Satterfield, 407-238-4161 (as of 5/12/2000)
Meniere's Disease Leads to a Significant Decline in
Quality of Life for Patients with Disorder
A University of California-San Diego study highlights disease's impact on physical and mental health
Orlando, FL -- Meniere's disease is a chronic illness that often affects individuals in the prime of life. Many believe the disorder has a serious impact on the psychosocial status of individuals and their families. For the first time, a new study quantifies health-related quality of life status of patients with Meniere's disease who have failed conventional medical therapy and are candidates for further intervention and compares their status with other medical disorders described in a similar fashion.
Early studies suggested that there was a psychosomatic component in the etiology of this disorder. Now, it is generally accepted that the psychological aspects of the illness are in fact the consequence of the disease itself. A number of studies have shown Meniere's disease is associated with anxiety, depression and inability to concentrate.
The authors of the study, "Impact of Meniere's Disease on Quality of Life," are Jeffrey P. Harris, MD, PhD, from the Division of Otolaryngology-Head & Neck Surgery, and John P. Anderson, PhD, Department of Family and Preventive Medicine, at the University of California-San Diego. Their findings were presented before the American Otologic Society, meeting May 13-15, in Orlando, FL.
Methodology: Nineteen patients (12 female, seven male, age 32 to 83 yrs); all had been diagnosed with Meniere's disease that had been resistant to medical therapy; the baseline interviews on the subjects were performed by trained interviewers prior to any medical intervention.
Three instruments were used in the study:
Quality of Well-being Scale (QWB): A quantitative general health measure that allows for comparison of all diseases or conditions. It permits an analysis of programs, policies and treatments for the specified diseases and conditions, and allows calculation of Quality-Adjusted Life Years gained or lost by affected individuals. Patients are asked about their experience and dysfunction for each of the past six consecutive days. They are asked to define their symptom/problem complex - (headache, dizziness, ringing in ears), using criteria such as mobility scale-e.g. limitations in travel, physical activity scale-e.g. in bed, and social activity scale- e.g. working, housework.
Medical Outcomes Study SF-12: Widely employed general health status measure. This research tool rates physical and mental status by asking how often or how troublesome described situations are either during the past week or ongoing.
Center for Epidemiologic Studies-Depression Scale (CES-D): This is a widely used measure of psychological depression. Generally, 20 items rated on a scale of 0-3 over the past week: zero (best) to 60 (worst). Scores 16 or above indicate clinically significant depression).
Results: The study revealed the following:
-- QWB scores: Meniere's patients achieved a mean score of .505 on days of acute episodes and .620 on days without acute episodes. This compares with scores of normal adults (.810), very ill adults with life-threatening illness (cancer, AIDS (.616), non-institutionalized Alzheimer's patients (.506), and AIDS & cancer patients, six days before death (.427). This indicates that Meniere's patients lost 43.9% from optimum well-being or .439 quality adjusted life years lost for each year in their QWB state. This score reflects major impairment in mobility, physical activity, social activity and clear thought processes.
-- CES-D scores: Meniere's patients registered a mean CES-D score of 23 (significant depression 16 and above). This compares with trauma patients (CES-D 20), cochlear implant candidates (CES-D 15), patients with post-cochlear implantation (CES- D 12).
-- SF-12 scores: Meniere's patients recorded scores SF-12 physical- 38.9 (mean 50, + 10) and SF-12 mental- 44.2 ( mean 50, + 10). Meniere's disease patients are among the most severely impaired non-hospitalized patients studied thus far. These patients exhibit even more impairment on days with acute episodes. Patients describe impairment in travel, ambulation, work and other major social roles as well as trouble learning, remembering and thinking clearly. They are clinically depressed as a group.
Conclusions: The degree of impairment and depression which stems from this condition becomes the responsibility of treating physicians to develop and offer treatment options to their Meniere's patients. The authors call on the medical community and fellow specialists to not condone a nihilistic approach to treatment, stress to primary care colleagues that this condition requires treatment, and seek out effective treatment strategies for this debilitating illness.
Saturday, February 2, 2013
Groundhog Day
Since it's February 2nd, I thought today would be the perfect day to explain how having Meniere's disease is a lot like Groundhog Day - the movie. If you've never seen it, here's the description over at Rotten Tomatoes:
Bill Murray plays Phil, a TV weatherman working for a local station in Pennsylvania but convinced that national news stardom is in his grasp. Phil displays a charm and wit on camera that evaporates the moment the red light goes off; he is bitter, appallingly self-centered, and treats his co-workers with contempt, especially his producer Rita (Andie MacDowell) and cameraman Larry (Chris Elliot). On February 2, 1992, Phil, Rita, and Larry are sent on an assignment that Phil especially loathes: the annual Groundhog Day festivities in Punxsutawney, PA, where the citizens await the appearance of Punxsutawney Phil, the groundhog who will supposedly determine the length of winter by his ability to see his own shadow. Phil is eager to beat a hasty retreat, but when a freak snowstorm strands him in Punxsutawney, he wakes up the next morning with the strangest sense of déjà vu: he seems to be living the same day over again. The next morning it happens again, and then again. Soon, no matter what he does, he's stuck in February 2, 1992; not imprisonment nor attempted suicide nor kidnapping the groundhog gets him out of the loop. But the more Phil relives the same day, the more he's forced to look at other people's lives, and something unusual happens: he begins to care about others. He starts to respect people, he tries to save the life of a homeless man, and he discovers that he's falling in love with Rita and therefore wants to be someone that she could love in return.
Comparison #1: Even when we're not feeling well, we have moments where we feel we must put on a happy face and act cheerful, just like Phil when the camera starts rolling, if only for a few moments at a time. Maybe if we do, the gods will shine down on us and reward our effort in some way. At the very least, maybe it will make us appear a little less like the grumpy jerks we feel like we've become. Feeling off-balance, unable to understand what people are saying to us, and being a stick in the mud of everyone else's fun when you're down with vertigo can add up to leaving us feeling bitter, appallingly self-centered, and treating our co-workers (or family and friends) with contempt.
Comparison #2: As we wake up each day, we look to our symptoms to hopefully predict what kind of day we will have. Will it be six more weeks of winter or will we be given a reprieve with an early spring? Like Phil, we can feel snowed in, stranded someplace we desperately want to escape. When we discover we can't escape, we try to imprison, slay, and kidnap the Beast to break the cycle we are stuck in.
While we might beat it back from time to time, the little critter remains insidious and persistent. Despite going weeks at a time feeling pretty normal and feeling like I have a handle on my emotions, that I will be able to cope better next time, even one bad day of feeling off-balance and brain foggy puts me right back to square one, emotionally. Every time. Exactly the way Phil feels when he wakes up each morning with deja vu. The kicker is that no one around him (us) has any idea that the same scenario keeps playing out, over and over. And over. And over... Everyone around us just goes on with their lives as if nothing is wrong.
Comparison #3: After awhile, despite the repetition of events that we just wish would cease once and for all, we must relent and face our reality. We will have good days, we will have bad days, and everyone around us will seem oblivious to our internal Groundhog Day. But once we embrace these facts, we can start to see little opportunities to feed our souls through the lives of those around us whose realities are thankfully different. We can begin to see that they are our rocks, our anchors. In turn, we can give whatever we can to them in return, however insignificant it might seem in comparison to what we'd like to be able to give. We can still love our family and friends and find ways to express that. And most importantly, we can rediscover that we are still lovable, by others and ourselves, despite our less than desirable disposition. I truly believe that embracing our limitations sets us free to go on living the best, most productive lives possible.
As you can imagine, Bill Murray and Chris Elliot are hysterical in Groundhog Day and it has a warm-fuzzy ending. Too bad our experience of living our own personal Groundhog Day isn't nearly as funny (though you can find humor in it sometimes), but we can still find warm-fuzzies if we open our eyes and hearts to them.
Bill Murray plays Phil, a TV weatherman working for a local station in Pennsylvania but convinced that national news stardom is in his grasp. Phil displays a charm and wit on camera that evaporates the moment the red light goes off; he is bitter, appallingly self-centered, and treats his co-workers with contempt, especially his producer Rita (Andie MacDowell) and cameraman Larry (Chris Elliot). On February 2, 1992, Phil, Rita, and Larry are sent on an assignment that Phil especially loathes: the annual Groundhog Day festivities in Punxsutawney, PA, where the citizens await the appearance of Punxsutawney Phil, the groundhog who will supposedly determine the length of winter by his ability to see his own shadow. Phil is eager to beat a hasty retreat, but when a freak snowstorm strands him in Punxsutawney, he wakes up the next morning with the strangest sense of déjà vu: he seems to be living the same day over again. The next morning it happens again, and then again. Soon, no matter what he does, he's stuck in February 2, 1992; not imprisonment nor attempted suicide nor kidnapping the groundhog gets him out of the loop. But the more Phil relives the same day, the more he's forced to look at other people's lives, and something unusual happens: he begins to care about others. He starts to respect people, he tries to save the life of a homeless man, and he discovers that he's falling in love with Rita and therefore wants to be someone that she could love in return.
Comparison #1: Even when we're not feeling well, we have moments where we feel we must put on a happy face and act cheerful, just like Phil when the camera starts rolling, if only for a few moments at a time. Maybe if we do, the gods will shine down on us and reward our effort in some way. At the very least, maybe it will make us appear a little less like the grumpy jerks we feel like we've become. Feeling off-balance, unable to understand what people are saying to us, and being a stick in the mud of everyone else's fun when you're down with vertigo can add up to leaving us feeling bitter, appallingly self-centered, and treating our co-workers (or family and friends) with contempt.
Comparison #2: As we wake up each day, we look to our symptoms to hopefully predict what kind of day we will have. Will it be six more weeks of winter or will we be given a reprieve with an early spring? Like Phil, we can feel snowed in, stranded someplace we desperately want to escape. When we discover we can't escape, we try to imprison, slay, and kidnap the Beast to break the cycle we are stuck in.
While we might beat it back from time to time, the little critter remains insidious and persistent. Despite going weeks at a time feeling pretty normal and feeling like I have a handle on my emotions, that I will be able to cope better next time, even one bad day of feeling off-balance and brain foggy puts me right back to square one, emotionally. Every time. Exactly the way Phil feels when he wakes up each morning with deja vu. The kicker is that no one around him (us) has any idea that the same scenario keeps playing out, over and over. And over. And over... Everyone around us just goes on with their lives as if nothing is wrong.
Comparison #3: After awhile, despite the repetition of events that we just wish would cease once and for all, we must relent and face our reality. We will have good days, we will have bad days, and everyone around us will seem oblivious to our internal Groundhog Day. But once we embrace these facts, we can start to see little opportunities to feed our souls through the lives of those around us whose realities are thankfully different. We can begin to see that they are our rocks, our anchors. In turn, we can give whatever we can to them in return, however insignificant it might seem in comparison to what we'd like to be able to give. We can still love our family and friends and find ways to express that. And most importantly, we can rediscover that we are still lovable, by others and ourselves, despite our less than desirable disposition. I truly believe that embracing our limitations sets us free to go on living the best, most productive lives possible.
As you can imagine, Bill Murray and Chris Elliot are hysterical in Groundhog Day and it has a warm-fuzzy ending. Too bad our experience of living our own personal Groundhog Day isn't nearly as funny (though you can find humor in it sometimes), but we can still find warm-fuzzies if we open our eyes and hearts to them.
Monday, January 28, 2013
Choices That People with Chronic Diseases Have to Make
As I've mentioned before, I follow quite a few blogs for inspiration, as well as for practical information. One of my favorite is Turning Straw into Gold, written by Toni Bernhard, J.D., for Psychology Today. Toni suffers from chronic fatigue syndrome, if I am not mistaken, and is also a long-practicing Buddhist. Her latest article, titled 5 Tough Choices You Face When Chronically Ill or in Pain, really articulates well the psychological agonizing we tend to put ourselves through on top of our physical ailment.
I encourage anyone with, or who loves someone with, a chronic illness to read the whole article, but I have listed Toni's 5 questions below followed by my own experience with each of them.
1. Do we talk openly about our health problems or do we keep them private?
I used to speak freely with just about anyone, sharing the fact that I have Meniere's disease and how it affects my life. By doing so, I found lots of compassion, support, and understanding. It also helped to explain why I tried not to over commit or that I might not always be able to keep the commitments I had made.
But this summer when I decided it was time to change jobs, I feared discrimination if I were to be open about my condition. So I didn't offer it up. I didn't lie, I just didn't confess anything either. I understand where employers are coming from, they don't want to invest money hiring and training an employee that has an increased risk of not being able to perform their duties or, god forbid, becoming disabled. On the other hand, I felt I was the best person to assess whether or not I could reliably do the job for which I was applying and not leave that up to a speculating employee health nurse or manager who has no clue about me or,most likely, this disease. I had not missed any work days in the past year or more and, since starting my new job six months ago, I have only called in sick once for an unrelated illness. Besides, there's no guarantee if, or when, my Meniere's symptoms will rear their ugly head again. It could be a very long time from now.
I apologize for going off on a tangent, but I think it helps to illustrate why I felt I had to do a 180 regarding my policy of transparency. Before this summer, I never thought I'd hide this aspect of myself from anyone, but then I had a change of heart. In one way, I feel guilty and I hate keeping secrets (my coworkers now understand I am hard of hearing and know I have a hearing aid, but I have been vague as to why), but I am also free of all speculation as to why I might seem under the weather some days or feel I am under the microscope for potentially making errors related to my episodic brain fog.
I don't go out of the way to hide anything about myself, I am still blogging, for instance, and someone could easily enough find it, but I am a little more private these days. I guess I have been afforded that luxury from the Meniere's gods - for the time being. And if word gets out, I'll cross that path when I come to it. At least I now have a record of good productivity and reliability with this new group of people.
2. Do we ignore a new symptom or have it checked out by a doctor?
For months, I attributed my poor cognition and near-constant fatigue to Meniere's. Then, being in my mid-forties, it dawned on me that I could have hypothyroidism or some other unrelated problem that might actually be treatable. Wow, what a concept - a medical condition that might have a treatment! So I made an appointment for a physical, had a whole panel of blood work done, and lo and behold... Nothing! But at least then I knew with relative certainty that indeed my issues were most likely related to This Stupid Disease after all.
Working with cancer patients as I do, I know all too well the consequences of ignoring insidious symptoms. But it's a fine line, as Toni elaborates on in the article.
3. Do we follow our doctor’s treatment plan or do we try alternative and unconventional therapies?
This is a tough one for anyone with Meniere's disease who has not responded to traditional medical treatment. I followed my doctor's advice to the letter. I took every pill, avoided salt like the plague, and kept all of my follow-up appointments, each timing reporting another failure in his well-laid plan. He was understanding, to say the least, but he also had little else to offer me, short of taking the next step with a destructive procedure (which I eventually did).
But before crossing that bridge, I ventured off the beaten path. I took a bucket load of supplements peddled by well-meaning individuals and racked up my credit card with chiropractic treatments. I don't regret either, but they helped me understand just how far this disease could push me toward desperation. I can't say I won't ever feel that desperate again. This is a miserable disease when at its worst.
4. Do we push our body to the limit or do we always play it safe?
Up until recently, I felt compelled to keep my life as normal as possible, living it as fully as my symptoms would allow. In other words, I lived up until the second the vertigo set in, being completely unable to think or walk. But last month I read another Meniere's sufferer's account of learning to cope with this Beast. His approach was to put the brakes on all activities at the first hint of an attack. This would be hours, or even days, ahead of when I would begin to slow down. I took his advice to heart and started to make myself take a break and meditate any time my tinnitus started ramping up or when I started to feel off-balance or brain foggy. It has made a big difference and I do think I may just have headed off a few attacks with this method.
My philosophy has been to not let Meniere's take away a minute more than absolutely necessary from my life, but now I realize I have to be proactive, too. By doing so, maybe I will get more of those good (aka vertigo-free) minutes for myself in the end.
5. Should we aggressively fight to regain our health or should we accept our fate?
I am a big believer that once we accept our circumstances new doors will magically open. If, on the other hand, we deny the obvious and simply wish things were different than they really are, it seems somehow that the powers of the universe know this and just needle us more.
What do you think of Toni's questions and how have you dealt with each of them?
Friday, January 25, 2013
Rock On, Dana White!
For those of you who don't know who Dana White is, he is the outspoken president of the Ultimate Fighting Championship (UFC) who also happens to have Meniere's disease. He has been very adamant about doing whatever necessary to control his vertigo and last week he underwent what appears to be endolymphatic shunt surgery at House Ear Clinic in Los Angeles. There have been several stories leading up to, including a video on YouTube of, his surgery.
Today this story was published quoting White on insisting on traveling, actually flying, less than a week after surgery despite being discouraged from doing so. Love this quote from him:
“It’s like me and my ear are two different people now,” White said. “My ear’s trying to make me do something that I don’t want to do and my ear is going to do what I want to f**king do. I’m in a personal fight every day with this f**king ear and I’m going to win, that’s how I look at it.”
Rock on, Dude!
Today this story was published quoting White on insisting on traveling, actually flying, less than a week after surgery despite being discouraged from doing so. Love this quote from him:
“It’s like me and my ear are two different people now,” White said. “My ear’s trying to make me do something that I don’t want to do and my ear is going to do what I want to f**king do. I’m in a personal fight every day with this f**king ear and I’m going to win, that’s how I look at it.”
Rock on, Dude!
Wednesday, January 23, 2013
More About Triggers
I saw this article on WebMD this evening. Sometimes their stuff is good and sometimes it is maddeningly paltry, containing no real substance to support some sensational headline. Those of you who follow my blog know I am not sold on there being reliable triggers for Meniere's symptoms based on my own personal experience anyway. Any Meniere's specialist worth his salt, however, will tell you to follow a diet, well, low in salt because it is thought to increase fluid in the inner ear and lead to symptoms. I plan to research the literature a bit to see how strong the evidence for this is because I've read it may actually be quite weak. Regardless, for the first two years after being diagnosed with Meniere's, I restricted my sodium intake religiously. In addition to those being the worst years of vertigo for me, trying to avoid sodium in my food certainly added to my overall poor quality of life during that time. This article touches on this very subject. Enjoy!
Tuesday, January 22, 2013
Hearing Loss and Mental Decline
Sometimes I read something that brings me to tears for the simple reason that I now know someone has validated what I have experienced, but couldn't necessarily articulate in words. This is an example of one of those times. But this is not just true in the elderly. I've often wondered if the brain fog I experience from time to time is directly linked to a fluctuation, a dip specifically, in my hearing. It just may be...
Hearing Loss Linked to Mental Decline in Elderly
Jan. 22, 2013 -- Hearing loss and mental decline are two common conditions of aging, and now a new study finds that they may be related.
Older people with hearing deficits were more likely than those with normal hearing to develop problems with memory and thinking over the course of the study.
On average, the study participants with hearing issues had significant mental impairments three years earlier than those without them.
Untreated Hearing Loss Common
About two-thirds of adults over the age of 70 have some degree of hearing loss.
And the number of people with dementia is projected to double over the next two decades as the population ages.
The researchers now hope to study whether hearing aids can slow mental decline in the elderly.
Otologist and epidemiologist Frank R. Lin, MD, PhD, led the study. He says only about 15% of people who need hearing aids get them. Lin is an assistant professor at the Johns Hopkins University School of Medicine in Baltimore.
“Our findings emphasize just how important it is for physicians to discuss hearing with their patients and to be proactive in addressing any hearing declines over time,” he says.
The investigation included close to 2,000 men and women in their 70s and 80s who took part in an aging and health study that began in the late 1990s.
Hearing was tested in year five of the study, and the men and women underwent a series of tests over the next six years to assess declines in memory and thinking.
The men and women with hearing loss showed evidence of these declines 30% to 40% faster than the people with normal hearing. And those people with more hearing loss had steeper declines in mental function.
The study was published online in the journal JAMA Internal Medicine.
Social Isolation, Brain Overload May Explain Link
While it did not address how age-related hearing loss may worsen problems with memory or thinking, Lin says there are several theories.
One theory is that the social isolation common among people with untreated hearing loss leads to mental decline. Previous research has identified loneliness as a risk factor for such decline, he says.
Another theory is the idea that the working memory is limited with respect to the amount of information it can hold and the operations it can perform.
“The job of the inner ear is to take in sounds and encode them with accurate fidelity before the signal goes to the brain for decoding, but with hearing loss the brain has a very hard time doing that,” Lin says. “If the brain constantly has to expend more resources to decode sound, this may come at a cognitive cost.”
Neurologist and Alzheimer’s researcher Marc L. Gordon, MD, calls the research compelling, but he says more studies are needed to confirm that hearing loss has a direct impact on mental decline and to understand the reasons for the link.
He adds that the study emphasizes the importance of addressing not just hearing loss but also vision loss in the elderly.
“This reinforces the notion that evaluating and treating these sensory impairments may be even more important for an aging person’s overall well-being than we have known,” he says.
http://www.webmd.com/healthy-aging/news/20130118/hearing-loss-mental-decline?src=RSS_PUBLIC
Monday, January 21, 2013
A Funny Story About Triggers
Anyone with Meniere's often wonders if there are any triggers which they should avoid in order to prevent attacks. Whether you visit websites with official medical advice or forums of Meniere's sufferers, you will certainly find a long list of plausible, and not so plausible, potential triggers which are thought to cause or worsen symptoms. To date, I've found few that hold true for me, most (inhaled allergens, for example) I have little control over so I try within reason not spend too much time worrying about them. But the mind is a funny thing.
As I work in healthcare, I am typically required each year by my employer to get a flu shot. However, I don't recall if I took one the past two winters or not because I did not have direct patient contact in my previous position, so for me getting a flu shot was optional. I think I may have opted out, not being entirely certain how it might affect my Meniere's symptoms. However this summer I changed employers and now as I do see patients face-to-face from time to time, I am again required to get immunized. As a general rule, I am fine with getting flu shots, not only to protect myself, but also my patients as most are quite immunocompromised.
Since I couldn't remember getting a flu shot in the past couple of years or what happened afterward, I worried a bit that it might mess with my current calm state of affairs. While I could technically opt-out by signing a waiver, I didn't want to create any waves since this new employer has no idea of my condition.
So several weeks ago after attending an off-site meeting where there happened to be an employee health office, I made my way over to it to take the plunge. As I walked up to the receptionist, I was a little nervous that I might be making a big mistake which I was going to regret. Despite the multiple email reminders I had already received from HR by that point, the receptionist kindly informed me that they had not yet started giving the shots. I was a day early! A little relieved, and a little miffed about the fact that coming back another day would be an incovenience, I went on my way.
Well, wouldn't you know it, but the next day I felt terrible. Roaring tinnitus, brain fog, and disequilibrium. These days this is what I consider a full-blown attack. But I just had to laugh because had I been able to get my flu shot the previous day, no doubt I would have attributed this attack to it.
This is a little lesson that before we assign triggers to our symptoms, we have to repeat the experiment several times to be sure. While this is not fun for sure, it is a necessary evil. The alternative is that we end up avoiding foods, activities, and other things that make our lives more enjoyable and healthier with the false belief that they trigger our symptoms. Meniere's already takes so much from us, we need to be careful not to be our own worst enemy, giving away all control of our circumstances to the Beast.
A few weeks later I finally got my flu shot and I am happy to report that I had no reaction whatsoever. With all the news of the current flu epidemic, I am glad to have a little extra protection on board and that I didn't let my fear get the best of me.
As I work in healthcare, I am typically required each year by my employer to get a flu shot. However, I don't recall if I took one the past two winters or not because I did not have direct patient contact in my previous position, so for me getting a flu shot was optional. I think I may have opted out, not being entirely certain how it might affect my Meniere's symptoms. However this summer I changed employers and now as I do see patients face-to-face from time to time, I am again required to get immunized. As a general rule, I am fine with getting flu shots, not only to protect myself, but also my patients as most are quite immunocompromised.
Since I couldn't remember getting a flu shot in the past couple of years or what happened afterward, I worried a bit that it might mess with my current calm state of affairs. While I could technically opt-out by signing a waiver, I didn't want to create any waves since this new employer has no idea of my condition.
So several weeks ago after attending an off-site meeting where there happened to be an employee health office, I made my way over to it to take the plunge. As I walked up to the receptionist, I was a little nervous that I might be making a big mistake which I was going to regret. Despite the multiple email reminders I had already received from HR by that point, the receptionist kindly informed me that they had not yet started giving the shots. I was a day early! A little relieved, and a little miffed about the fact that coming back another day would be an incovenience, I went on my way.
Well, wouldn't you know it, but the next day I felt terrible. Roaring tinnitus, brain fog, and disequilibrium. These days this is what I consider a full-blown attack. But I just had to laugh because had I been able to get my flu shot the previous day, no doubt I would have attributed this attack to it.
This is a little lesson that before we assign triggers to our symptoms, we have to repeat the experiment several times to be sure. While this is not fun for sure, it is a necessary evil. The alternative is that we end up avoiding foods, activities, and other things that make our lives more enjoyable and healthier with the false belief that they trigger our symptoms. Meniere's already takes so much from us, we need to be careful not to be our own worst enemy, giving away all control of our circumstances to the Beast.
A few weeks later I finally got my flu shot and I am happy to report that I had no reaction whatsoever. With all the news of the current flu epidemic, I am glad to have a little extra protection on board and that I didn't let my fear get the best of me.
Friday, January 18, 2013
Coping with an Uncertain Future
If there's one thing everyone with Meniere's Disease has in common, it is the first-hand, brutal understanding that life is uncertain.
Before Meniere's, I had no problem making plans days, weeks, even years in advance with confidence. Today I still make most of those plans, but with the understanding that everything in life is tentative. I hope I can keep my commitments, but I won't be devastated if I can't. Life, it turns out, goes on anyway. It's an interesting way to live, to say the least. It would be easy to succumb to fear under these circumstances as no one wants to let others down.
The fear of suffering is worse than the suffering itself. ~Paulo Coelho
Instead I've learned to embrace this knowledge as a positive thing because isn't it true that no one's future is guaranteed? At least those of us with Meniere's know this already and so when things don't go as we'd hoped, it's not such a shock.
Sometimes not getting what we want is a wonderful stroke of luck. ~Dalai Lama
I read several inspirational blogs and lean on others for support who happen to be traveling this journey with me. While skimming Tiny Buddha the other day, I came across Lisa H.'s blog, Getting to Zen, and her post Finding Peace When You Feel Scared About What Might Happen. As I was reading about her experience of how she coped while waiting for the results of a breast biopsy (everything turned out to be okay), I couldn't help but see the parallels between this and the experience of living with Meniere's.
For those who don't know, the symptoms of Meniere's disease are episodic and unpredictable. This can be the most frustrating, and fearful, part of the condition, since you simply cannot know when an attack might occur or just how disabling it will be. Not only that, but one might go weeks, months, or years doing very well. They might even think they're "cured", only to be knocked down again completely out of the blue. There's no rhyme or reason to it. A certain percentage of people, statistics vary from 5-50%, eventually become significantly and permanently disabled. So even as I breeze though this time of reprieve, I live everyday with these statistics in my head and the images conjured up from reading the accounts of those who are living through the worst of it - usually from bed or a wheelchair, their hearing limited to the roaring of constant, load tinnitus. One study actually found that the quality of life rated by people living with advanced Meniere's disease is worse than that of people with AIDS or cancer in the last six days of life. So for those of us with this disease it is no joke to have to learn to cope with the fear of the future.
I'd like to borrow from Lisa H.'s advice and tailor it to the Meniere's experience:
Limbo is not a bad place.
Living with not knowing what the future holds, or even with suffering in the moment, has taught me that the present moment is never intolerable. We make our present intolerable by placing conditions on it. For example, during an attack when I've been confined to bed for hours at a time, waiting for the room to stop spinning, yes, it is physically very uncomfortable. But it is far worse when my thoughts revolve around what I should be doing. "I should be at work. Everyone must be so mad at me for having to take on my responsibilities." "My kids must be so sad I cannot pick them up from school today." Instead, by gently bringing my mind and thoughts back around to the exact present moment I remind myself to embrace it as it is and deal head-on with what I am living. There are some things we just cannot control, no matter how much we wish we could.
Try not to worry.
I cannot add to Lisa's words, they are perfect. She says:
Worrying is useless. It serves absolutely no purpose. The past is gone and the future hasn't happened yet. Don't use your present time worrying about things you can't control.
She goes on to say, Instead of worrying, meditate, practice gratitude, become still, listen to your soul, and surround yourself with love. Yes!
Nothing is permanent.
This is so true of what living with Meniere's is like. There are very dark days where you are certain this is how you will feel for the rest of your life. The vertigo, disequilibrium, hearing loss, and deep fatigue can last hours or come and go in rapid succession for weeks or months on end. But they always change in intensity and eventually frequency. Not only do the symptoms change, but so can our perception of what they mean to us. Many of us also experience periods of normal life when we can almost forget we even have this cross to bear.
When I was first diagnosed, my doctor made a horrifying comment to me. He said, "We consider you well-managed if you have less than two or three episodes of vertigo a year." At the time, I couldn't believe I could possibly live with having two or three horrific vertigo attacks every year. That was simply unacceptable to me. If I had only known how much worse things would get before they got better. In hindsight, I am so glad I didn't know. I went on to have two or three of these attacks every week off and on for the next two years. My, how my perception of things changed during since time.
It is okay to be afraid.
I found a lot of my own suffering was caused by trying to manage my fear. Eventually, I learned to embrace it. By admitting I was afraid, I acknowledged how that felt and learned that it would not kill me. Fear is often caused by uncertainty. As it turns out, life for everyone is uncertain yet we cannot be paralyzed with fear. At least now, I fully understand what that means and I am okay with it.
Surround yourself with love.
Again, Lisa H.'s words mirror what I have learned from living with chronic illness.
Let those close to you know what is going on in your life and how you feel about it. There is no need to carry the weight of a challenge on your own. Sometimes hearing others talk can shed light on what would otherwise be a bleak situation.
One thing I have learned is that sharing that I have Meniere's disease with others and what it means for me can be a double-edge sword. On the one hand, letting family and close friends know what is going on can help explain why you seem unreliable or distant and allow them to support you. It will prevent people from speculating, incorrectly, about what might be going on. On the other hand, once you share the information with say acquaintances or co-workers, you can never take it back and it might come back to haunt you later. You might know what you're capable of taking on, but those who don't know you well might doubt your abilities to complete a project, for example. Yet again, by not sharing your situation with others, you might rob yourself of support and opportunities to learn about their challenges and how they've coped.
Deciding who to share your illness with and when must be made on a case by case basis.
Take care of yourself.
This is a constant challenge when living with Meniere's disease. Many people find that stress and overdoing it often makes them feel worse. Yet when we are feeling well, we want to be "normal" again and live each day to the fullest.
I have settled into certain habits that I try to stick to everyday which help minimize my anxiety and promote good physical health. I eat three meals a day and limit my intake of processed food. I drink water often. I make sure to set aside eight to nine hours for sleep each night. I limit my commitments. I meditate for at least a few minutes every night before I go to sleep. I seek out inspiring stories and quotes to reflect on. And, perhaps most importantly, I find things in my life every day, no matter how awful I feel, to be grateful for. Even it is just for the roof over my head and the soft bed cradling my body, I still remember that there's always someone out there who is worse off than me.
You are always going to be okay.
The older we get, the more opportunities we've had to experience something we fear. We all have things that we think, "If that ever happened to me, I'd just die." Well, sadly sometimes those things do happen and guess what? We don't die. In fact, sometimes we come away learning that we were stronger than we thought. We find that we must reevaluate our expectations and adjust them in order to accommodate things that we simply don't have any control over. We learn to identify, manage, and focus on the things we can control.
In the end, that's a beautiful thing.
Before Meniere's, I had no problem making plans days, weeks, even years in advance with confidence. Today I still make most of those plans, but with the understanding that everything in life is tentative. I hope I can keep my commitments, but I won't be devastated if I can't. Life, it turns out, goes on anyway. It's an interesting way to live, to say the least. It would be easy to succumb to fear under these circumstances as no one wants to let others down.
The fear of suffering is worse than the suffering itself. ~Paulo Coelho
Instead I've learned to embrace this knowledge as a positive thing because isn't it true that no one's future is guaranteed? At least those of us with Meniere's know this already and so when things don't go as we'd hoped, it's not such a shock.
Sometimes not getting what we want is a wonderful stroke of luck. ~Dalai Lama
I read several inspirational blogs and lean on others for support who happen to be traveling this journey with me. While skimming Tiny Buddha the other day, I came across Lisa H.'s blog, Getting to Zen, and her post Finding Peace When You Feel Scared About What Might Happen. As I was reading about her experience of how she coped while waiting for the results of a breast biopsy (everything turned out to be okay), I couldn't help but see the parallels between this and the experience of living with Meniere's.
For those who don't know, the symptoms of Meniere's disease are episodic and unpredictable. This can be the most frustrating, and fearful, part of the condition, since you simply cannot know when an attack might occur or just how disabling it will be. Not only that, but one might go weeks, months, or years doing very well. They might even think they're "cured", only to be knocked down again completely out of the blue. There's no rhyme or reason to it. A certain percentage of people, statistics vary from 5-50%, eventually become significantly and permanently disabled. So even as I breeze though this time of reprieve, I live everyday with these statistics in my head and the images conjured up from reading the accounts of those who are living through the worst of it - usually from bed or a wheelchair, their hearing limited to the roaring of constant, load tinnitus. One study actually found that the quality of life rated by people living with advanced Meniere's disease is worse than that of people with AIDS or cancer in the last six days of life. So for those of us with this disease it is no joke to have to learn to cope with the fear of the future.
I'd like to borrow from Lisa H.'s advice and tailor it to the Meniere's experience:
Limbo is not a bad place.
Living with not knowing what the future holds, or even with suffering in the moment, has taught me that the present moment is never intolerable. We make our present intolerable by placing conditions on it. For example, during an attack when I've been confined to bed for hours at a time, waiting for the room to stop spinning, yes, it is physically very uncomfortable. But it is far worse when my thoughts revolve around what I should be doing. "I should be at work. Everyone must be so mad at me for having to take on my responsibilities." "My kids must be so sad I cannot pick them up from school today." Instead, by gently bringing my mind and thoughts back around to the exact present moment I remind myself to embrace it as it is and deal head-on with what I am living. There are some things we just cannot control, no matter how much we wish we could.
Try not to worry.
I cannot add to Lisa's words, they are perfect. She says:
Worrying is useless. It serves absolutely no purpose. The past is gone and the future hasn't happened yet. Don't use your present time worrying about things you can't control.
She goes on to say, Instead of worrying, meditate, practice gratitude, become still, listen to your soul, and surround yourself with love. Yes!
Nothing is permanent.
This is so true of what living with Meniere's is like. There are very dark days where you are certain this is how you will feel for the rest of your life. The vertigo, disequilibrium, hearing loss, and deep fatigue can last hours or come and go in rapid succession for weeks or months on end. But they always change in intensity and eventually frequency. Not only do the symptoms change, but so can our perception of what they mean to us. Many of us also experience periods of normal life when we can almost forget we even have this cross to bear.
When I was first diagnosed, my doctor made a horrifying comment to me. He said, "We consider you well-managed if you have less than two or three episodes of vertigo a year." At the time, I couldn't believe I could possibly live with having two or three horrific vertigo attacks every year. That was simply unacceptable to me. If I had only known how much worse things would get before they got better. In hindsight, I am so glad I didn't know. I went on to have two or three of these attacks every week off and on for the next two years. My, how my perception of things changed during since time.
It is okay to be afraid.
I found a lot of my own suffering was caused by trying to manage my fear. Eventually, I learned to embrace it. By admitting I was afraid, I acknowledged how that felt and learned that it would not kill me. Fear is often caused by uncertainty. As it turns out, life for everyone is uncertain yet we cannot be paralyzed with fear. At least now, I fully understand what that means and I am okay with it.
Surround yourself with love.
Again, Lisa H.'s words mirror what I have learned from living with chronic illness.
Let those close to you know what is going on in your life and how you feel about it. There is no need to carry the weight of a challenge on your own. Sometimes hearing others talk can shed light on what would otherwise be a bleak situation.
One thing I have learned is that sharing that I have Meniere's disease with others and what it means for me can be a double-edge sword. On the one hand, letting family and close friends know what is going on can help explain why you seem unreliable or distant and allow them to support you. It will prevent people from speculating, incorrectly, about what might be going on. On the other hand, once you share the information with say acquaintances or co-workers, you can never take it back and it might come back to haunt you later. You might know what you're capable of taking on, but those who don't know you well might doubt your abilities to complete a project, for example. Yet again, by not sharing your situation with others, you might rob yourself of support and opportunities to learn about their challenges and how they've coped.
Deciding who to share your illness with and when must be made on a case by case basis.
Take care of yourself.
This is a constant challenge when living with Meniere's disease. Many people find that stress and overdoing it often makes them feel worse. Yet when we are feeling well, we want to be "normal" again and live each day to the fullest.
I have settled into certain habits that I try to stick to everyday which help minimize my anxiety and promote good physical health. I eat three meals a day and limit my intake of processed food. I drink water often. I make sure to set aside eight to nine hours for sleep each night. I limit my commitments. I meditate for at least a few minutes every night before I go to sleep. I seek out inspiring stories and quotes to reflect on. And, perhaps most importantly, I find things in my life every day, no matter how awful I feel, to be grateful for. Even it is just for the roof over my head and the soft bed cradling my body, I still remember that there's always someone out there who is worse off than me.
You are always going to be okay.
The older we get, the more opportunities we've had to experience something we fear. We all have things that we think, "If that ever happened to me, I'd just die." Well, sadly sometimes those things do happen and guess what? We don't die. In fact, sometimes we come away learning that we were stronger than we thought. We find that we must reevaluate our expectations and adjust them in order to accommodate things that we simply don't have any control over. We learn to identify, manage, and focus on the things we can control.
In the end, that's a beautiful thing.
Monday, January 14, 2013
Time for Reflection
Every three months I make the 2-1/2 hour drive from San Diego to the House Ear Clinic, just west of downtown Los Angeles, to see Dr. Derebery who is a Meniere's and allergy specialist. It's not a terrible drive, just long and lonely. No matter what I listen to on the radio, each time I tend to reflect on my Meniere's journey at some point. It usually starts with some "poor me"-ing for having to spend so many hours in the car. But pretty quickly it turns to sheer amazement at how far I've come and gratitude that I am only a few hours from one of the best doctors in the country for treating this disease.
Today I reflected on the progress I've made thanks to two particular treatments: intratympanic (IT) gentamicin and allergy shots. Two years ago, I was in bad shape and had little hope that anything would ever relieve the relentless vertigo I was having after failing just about every noninvasive, nondestructive treatment. Most doctors, and even other Meniere's sufferers, strongly advise against doing anything destructive without first exhausting all other options. While I don't disagree, I also know firsthand how incessent episodes of vertigo can bring life to a screeching halt. Even if I'd known then what I know now, specifically that I had allergies and that treating them with desensitation therapy, aka allergy shots, would eventually help me gain control over this disease, I still think I would have taken the gent first.
Gent is quick and dirty. Yes, it causes permanent vestibular and, in a small percentage of cases, hearing loss, but it stopped the vertigo for me in a matter of weeks. Allergy shots, on the other hand, took three to six months to begin to produce consistent relief. A year later, my episodes of brain fog, dysequilibrium, and fatigue are much shorter, usually lasting just a few days or less, and much farther in between - three to six weeks or more. My quality of life has been so much better these past six months than any time since this dreaded disease took hold of me nearly four years ago.
I do wish I had known from the very beginning what I know now. But, hey, that's never how life works, is it? In the meantime, I've grown and matured into a different and better person. I don't think time lost to physical or emotional suffering has to be time wasted. I have learned that life is not always in my control and I can now accept that. I certainly did not know or believe that before in the most intimate way I do now.
Today, I sat in the busy waiting room at House and observed the clinic's other patrons. They ranged in age from a few years old to the very elderly and everything in between. They had walkers, wheelchairs, and cochlear implants. Some wore happy faces and others had looks of despair that I can only surmise came from suffering in one way or another from a hearing and/or vestibular disorder. I could only hope for them that they, too, might soon find relief from whatever was troubling them.
I don't know what tomorrow will bring, but I am so grateful for today. Thanks to Meniere's, I am reminded that these days may not be endless and that another round of Meniere's-related, or other, suffering could be right around the corner. That's okay. I'll deal with it if and when it comes.
Paulo Coelho, one of my favorite authors, said it best:
"The fear of suffering is worse than the suffering itself."
Today I reflected on the progress I've made thanks to two particular treatments: intratympanic (IT) gentamicin and allergy shots. Two years ago, I was in bad shape and had little hope that anything would ever relieve the relentless vertigo I was having after failing just about every noninvasive, nondestructive treatment. Most doctors, and even other Meniere's sufferers, strongly advise against doing anything destructive without first exhausting all other options. While I don't disagree, I also know firsthand how incessent episodes of vertigo can bring life to a screeching halt. Even if I'd known then what I know now, specifically that I had allergies and that treating them with desensitation therapy, aka allergy shots, would eventually help me gain control over this disease, I still think I would have taken the gent first.
Gent is quick and dirty. Yes, it causes permanent vestibular and, in a small percentage of cases, hearing loss, but it stopped the vertigo for me in a matter of weeks. Allergy shots, on the other hand, took three to six months to begin to produce consistent relief. A year later, my episodes of brain fog, dysequilibrium, and fatigue are much shorter, usually lasting just a few days or less, and much farther in between - three to six weeks or more. My quality of life has been so much better these past six months than any time since this dreaded disease took hold of me nearly four years ago.
I do wish I had known from the very beginning what I know now. But, hey, that's never how life works, is it? In the meantime, I've grown and matured into a different and better person. I don't think time lost to physical or emotional suffering has to be time wasted. I have learned that life is not always in my control and I can now accept that. I certainly did not know or believe that before in the most intimate way I do now.
Today, I sat in the busy waiting room at House and observed the clinic's other patrons. They ranged in age from a few years old to the very elderly and everything in between. They had walkers, wheelchairs, and cochlear implants. Some wore happy faces and others had looks of despair that I can only surmise came from suffering in one way or another from a hearing and/or vestibular disorder. I could only hope for them that they, too, might soon find relief from whatever was troubling them.
I don't know what tomorrow will bring, but I am so grateful for today. Thanks to Meniere's, I am reminded that these days may not be endless and that another round of Meniere's-related, or other, suffering could be right around the corner. That's okay. I'll deal with it if and when it comes.
Paulo Coelho, one of my favorite authors, said it best:
"The fear of suffering is worse than the suffering itself."
Tuesday, January 1, 2013
Meniere's, Migraine, and Bilateral Disease
I just came across this article about a recently published study which found a higher rate of bilateral Meniere's in people with a history of migraine. It only suggests correlation, but it is interesting nevertheless. Here's the story:

Study: Family History, Migraines Found Linked to Meniere's Disease
Posted on: December 30, 2012
In Otology & Neurotology, researchers from the University of Pennsylvania, Philadelphia, found patients with bilateral Meniere's Disease (MD) have a higher incidence of migraines and of a family history of MD. MD is based on the presence of vertigo, sensorineural hearing loss, tinnitus and aural fullness.
Their study appeared in the journal Otology & Neurotology.
The authors prospectively evaluated 224 patients with MD, 31 had bilateral disease. They report the average age of onset for their unilateral MD patients was 46.6 years (+/- 12.5 years) and for their patients with bilateral MD, the average age of onset was 39.9 years (+/- 13.8 years), yielding a statistically significant difference in the age at onset for the two groups (unilateral vs. bilateral MD). However, the exact diagnostic criteria for unilateral and bilateral MD are variable and the etiology remains unknown.
Of note, the co-morbidity of MD and migraine is historically reported to range from 22 to 56 percent. However, they authors noted with respect to their patients with unilateral MD, only 10% report a history of migraines, while 41% of their patients with bilateral MD indicated a history of migraine.
With regard to a family history of MD, only 4% of the patients with unilateral, and 28 percent of the patients with bilateral, Meniere's Disease reported a positive family history of MD. The authors report that in typical bilateral MD cases, the second ear may present with MD many years (ranging from 0 to 30 years) after the first ear.
|
Subscribe to:
Posts (Atom)